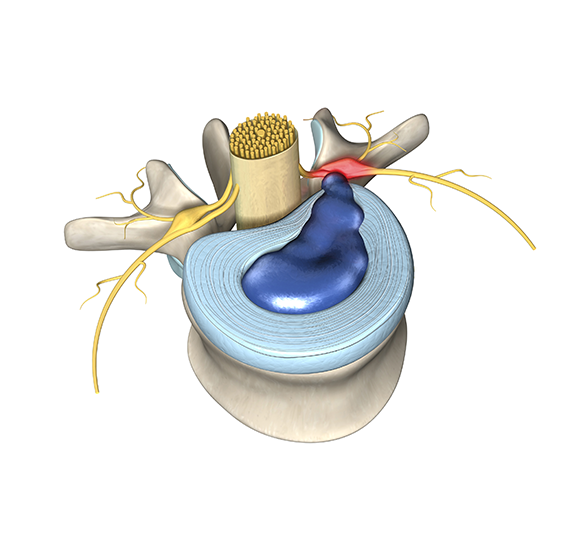

The #1 MISTAKE Back Pain Sufferers Make
By Dan Lieberman, MD In medicine the right treatment depends on understanding exactly what is wrong. The challenging thing about the lower back is that there are so many different problems, and even more treatments. In addition, the stakes are high. It is NOT just about relieving your pain; the wrong treatment is risky, sucks [...]
read more