The Best Spinal Fusion Surgeons in Gilbert AZ and the East Valley
Spine fusion is a highly effective, safe and reliable surgical procedure to relieve low back and neck pain caused by spondylolisthesis and instability. However, spine fusion is major surgery. And not all surgeons do it well. To stay safe and have a great result there is nothing you can do as a patient more vital than picking the best spinal fusion surgeon.
This page will give you the basics of spinal fusion surgery and recovery, and the Best Practice standards for selecting the best doctor for you. We will then introduce you to the surgeons in Gilbert and the East Valley that our team at Best Practice Health has identified as best qualified for spine fusion surgery. We do not cover neck fusion (Anterior Cervical Discectomy and Fusion) on this page. Look for upcoming posts on ACDF.
The early Symptoms of Spinal Stenosis
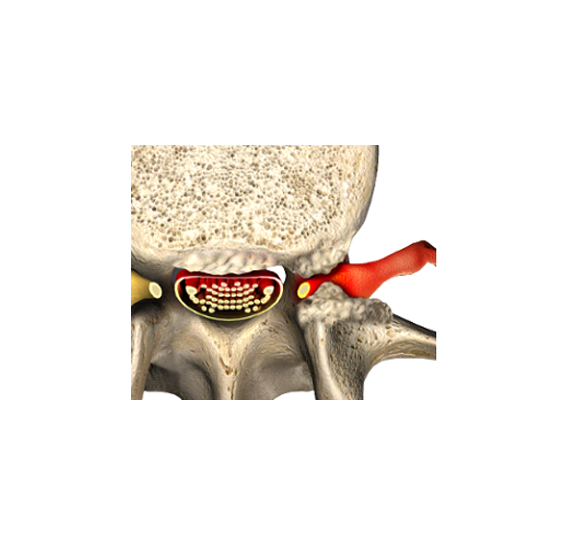
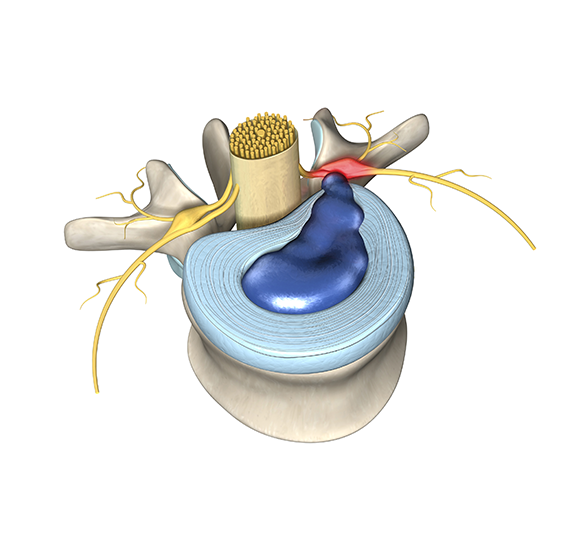
Spine fusion relieves severe pain in the lumbar spine and sciatica caused by instability, but more commonly spinal fusion is required for spondylolisthesis with stenosis. Spinal fusion is also done for scoliosis, a spinal deformity; however, that type of fusion is not covered on this page. (In the East Valley see Dr. Dennis Crandall for all cases of adult scoliosis deformity of the spinal column.) Instability in the spine is abnormal movement resulting from spinal fractures, degeneration or rare spine conditions like tumor or bone infections. In spondylolisthesis, one spinal bone slips compared to its neighbor, often causing narrowing in the spinal canal (stenosis) and pinched nerve roots.
There are 3 approaches to spine fusion in the low back depending on the level affected. This is important because the different approaches have levels of invasiveness and risk of permanent nerve damage. Double check that any surgeon who proposes fusion plans to use the approach described for the level you need or explain why not.
Approaches of Spinal Fusion
Spine fusion can be done using three different surgical approaches: from the back (posterior lumbar interbody fusion, PLIF), the front (anterior lumbar interbody fusion, ALIF) or the side. The optimal approach depends mostly on the level of the spine being fused. Surgery from the front (ALIF) is the preferred approach for the L5/S1.
The PLIF & TLIF procedures, done from the back, are basically the same thing. These approaches should be done using a minimally invasive approach. Your surgeon needs to be trained, experienced, and expert at microsurgery to properly execute this operation.
At the L3/4 level the TLIF approach risks causing permanent weakness to the quadriceps muscle which can prevent proper walking. At L3/4 the best approach is therefore from the side. Surgery at the remaining level is rare.
| Approach | |
|---|---|
| L5/S1 | Anterior Lumbar Interbody Fusion (ALIF) |
| L4/5 | Posterior / Transforaminal Interbody Fusion (PLIF or TLIF) |
| L3/4 | Lateral lumbar interbody fusion |
Minimally Invasive Spine Surgery
Spinal fusion can be done through two surgical techniques. While the traditional technique may be easier for the surgeon, the newer minimally invasive spine surgery technique makes the process easier for you.
The traditional technique is easier for the surgeon but requires opening the spine and permanently damages muscle. With minimally invasive spinal fusion, the procedure is done through a microscope or endoscope. This preserves your muscles, reduces the risk of infection, and it can lead to faster recovery. Because minimally invasive surgery is less painful you also do not need to go to a hospital. Having surgery in an ambulatory surgery center eliminates your risk of hospital errors and greatly lowers the risk of staph infection.
Risks of Spinal Fusion Surgery
As with any surgery, there are other risks to consider when getting spinal fusion and methods to reduce them.
The most likely complication of spinal fusion surgery is pedicle screw misplacement. This occurs in up to a third of spinal fusion cases, but it can be avoided with computer navigation and intraoperative imaging.
Failed low back surgery syndrome with persistent pain can also occur due to permanent weakness and spine damage caused by the traditional approach. The bone graft applied at surgery may not heal properly. The risk of failed low back surgery syndrome can be reduced with minimally invasive surgical techniques, which also significantly reduce the risk of infection and blood clots.
The most morbid risk of spinal fusion surgery as mentioned above is nerve root damage (spinal cord injury is not a risk in the lower back). This can be largely avoided by selecting a well trained and experienced surgeon as well as taking the approaches listed above at the appropriate levels.
Best Practice Recommendations for Spinal Fusion Surgeons
Best Practice Health’s recommendation for spinal fusion techniques is the use of retractors (like Medtronic Metrx) and magnification (microscope or endoscope) that allows surgeons to operate through tiny incisions and spare normal muscle and tendons, thereby leaving the spine stronger. They also make recovery faster and surgery less painful.
Additionally, navigational guidance and intra-operative imaging should be used to further reduce risks.
Finally, your surgeon should be appropriately trained and experienced. Training is confirmed by Board Certification in Orthopedic or Neurosurgery. The orthopedic surgeons should also have completed a fellowship year specializing in spinal surgery.
Recovery for Spinal Fusion Surgery
Recovery after spinal surgery varies depending on individual circumstances. Spinal fusion surgery is usually a quick procedure that is finished within a couple of hours. Patients need some time to recover from anesthesia but are generally able to go home the same day.
You will usually be asked to take a 10 minute walk each day for a week after surgery, 20-minute walks during the second week and 30-minute walks during the third. At that point, you will likely begin exercises to strengthen your core.
The healing process may come with some pain and discomfort, but you should expect your level of pain to decrease as you recover.
Surgical approach also matters, and getting invasive spine surgery can also impact recovery time. The timeline of your recovery depends on the activity level of your lifestyle. You will be able to return to light activity within three weeks, heavy duty work within 12 weeks and with surgeon approval.
Choosing Your Surgeon
Best Practice only certifies surgeons who are the best at the surgeries they perform.
Best Practice Health Certified Spinal Fusion Surgeons - East Valley, AZ
[insurancefilter class=”grid_insurance” layout=”slider” joint=”Back” default_pro=”Low back fusion (1 level)” location=”Gilbert, AZ” miles=”10″]
Spinal Fusion Surgery FAQs:
Hopefully our article has given you the tools you need to start picking the best spinal fusion surgeon for you. Here are some additional questions patients frequently have about spinal fusion surgery.
How long is a hospital stay after spinal fusion?
This is a trick question! With minimally invasive techniques and intraoperative navigational guidance, no hospital stay is needed. These operations can usually be done as an outpatient procedure in an ambulatory surgery center. This helps avoid the risk of hospital staph infections or potentially fatal hospital errors.
Will I be able to drive again after spinal fusion surgery?
Yes, but it depends when. It’s up to your surgeon, but most allow you to drive when you are weaned off narcotics one to two weeks after surgery. With minimally invasive surgical techniques, however, you may not need narcotics at all.
How long does it take to walk after spinal fusion surgery?
You should be able to walk out of the ambulatory surgery center four to five hours after you arrive. Although you will be able to walk, be sure to take it easy in the days after surgery and closely follow your surgeon’s instructions.